The Two Types of Shoulder Impingement — And Why One Responds Better to Rehab
👋 A Common Cause of Shoulder Pain
Shoulder impingement is one of the most common reasons people come to clinic — accounting for up to 65% of shoulder problems. But not all impingement is the same. To get better, you need to know what’s really going on.
If you’re new to the idea of shoulder impingement or want to understand the basics first, check out our previous article on symptoms, diagnosis, and how osteopathy can help:
👉 Shoulder Impingement: Symptoms, Treatment, and Expert Care in Manchester
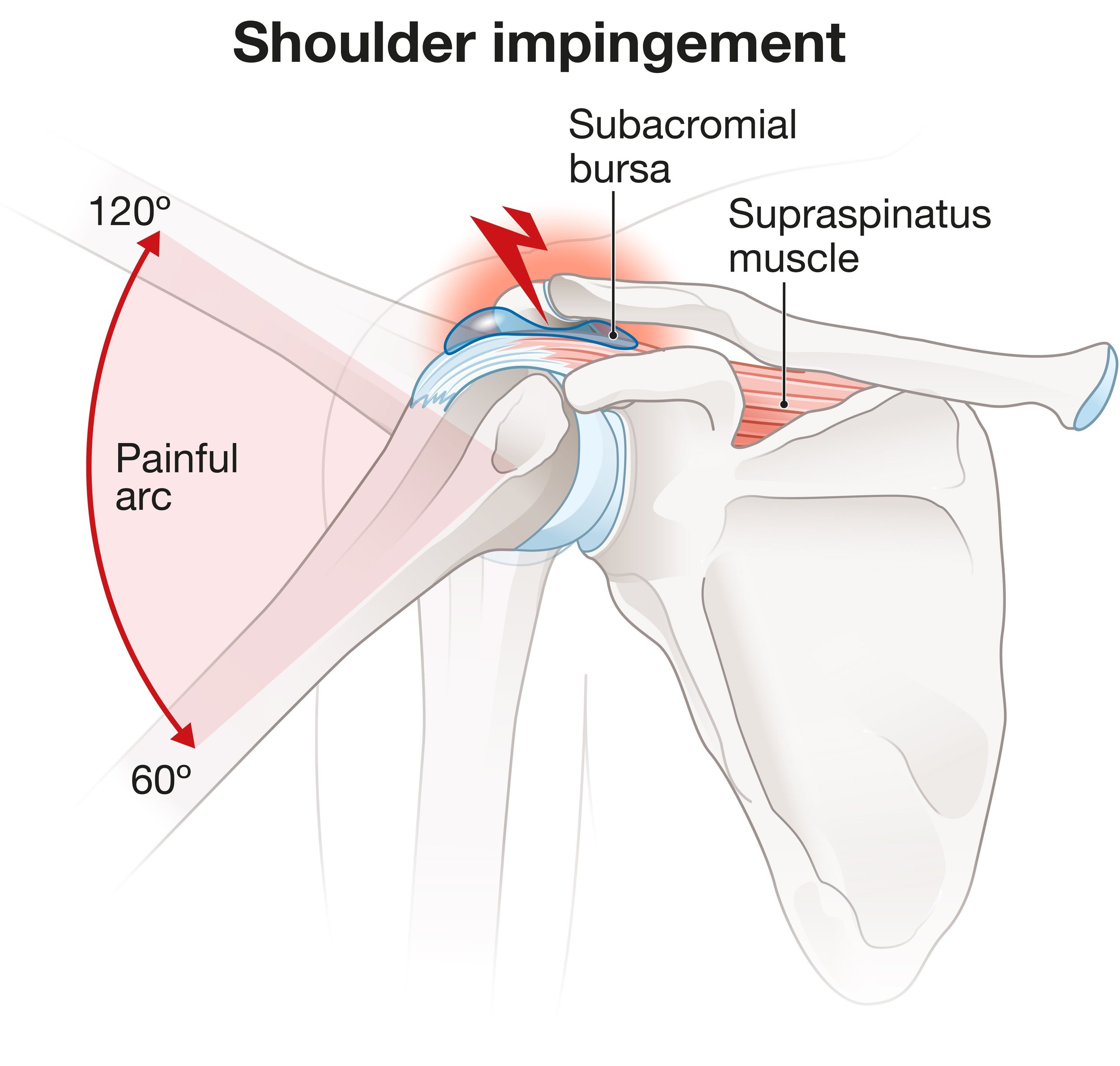
This is an example of external shoulder impingement
🔍 External vs Internal Impingement — What's the Difference?
External impingement (aka subacromial) happens outside the shoulder joint. It's when tendons or soft tissue get pinched between the top of your arm bone and the bony shelf above (the acromion).
Usually felt in movements like lifting the arm or reaching overhead.
Involves tendons like the supraspinatus or structures like the bursa.
Internal impingement happens within the shoulder joint. It tends to affect people who use their arms in overhead positions — like tennis players or swimmers.
The rotator cuff gets pinched inside the joint itself, between the head of the humerus and the glenoid rim, during certain movements like serving or throwing.
⚙️ Primary vs Secondary — Structure or Movement?
You can also think of impingement in terms of cause:
Primary impingement is often structural. Think of it as a shoulder that’s built a little narrower or has bony changes (like a hooked acromion) or thickened tissues. These issues create less space for tendons to move freely.
Secondary impingement is more about how you move. Poor shoulder blade control, weak rotator cuff muscles, or hypermobility can all lead to the arm bone drifting into the wrong place during motion — narrowing the space dynamically.
✅ The good news? Secondary impingement responds really well to rehab.
🧠 Real-Life Example
Imagine a recreational tennis player in their 50s. They’ve developed some age-related changes in the shoulder joint (primary issue), but they’ve also lost strength in their rotator cuff and control of their shoulder blade (secondary issue). The structure sets the stage, but poor movement patterns trigger the pain.
🔄 What Can Be Done?
For primary impingement, things like bony shape can’t be changed easily — but we can often reduce inflammation and improve the way the shoulder functions.
For secondary impingement, treatment works best when it includes:
Strengthening the rotator cuff — especially supraspinatus and infraspinatus.
Improving scapular control — with exercises for trapezius and serratus anterior.
Posture and mobility work — to create more space and ease stress on the joint.
And no, you don’t always need scans. A detailed assessment can usually give us a very clear picture.
⚠️When to Get a Second Opinion
No improvement after 6–8 weeks of rehab
Sudden loss of shoulder strength
Night pain that keeps getting worse
Severe stiffness or trouble rotating the shoulder
Final Thoughts
Shoulder impingement isn't one-size-fits-all. Whether it's structural, functional, or a bit of both — understanding the why behind the pain is key to long-term improvement.
👉 If your shoulder’s been nagging or holding you back, get in touch. A proper assessment can help you get clarity and a plan that works.